|
I had an exchange on Twitter with people alleging that doctors are finding that the drug hydroxychloroquine is 100% effective against COVID-19 and posting videos of patients claiming they had been cured by this drug. I tried to explain that this evidence is not valid and provided a link to one of my previous posts that addressed these claims. Then I stated that we need to wait for the results of the clinical trials. The response I got was that if doctors and their patients have tried it and are convinced it works, then that’s all the evidence we need. Unfortunately, this is simply not true. Even before hydroxychloroquine came along, the majority of patients hospitalized with COVID-19 would survive. If all patients are treated with hydroxychloroquine, then how do we know which patients got better because of the drug and which got better because they were going to get better anyway, or because of other treatments? In an uncontrolled clinical environment in the middle of a pandemic, patients are not randomized into matched groups and their treatments controlled and blinded to exclude placebo effects and other biases. Patient testimonials and doctor’s opinions are valuable to design clinical trials, but they have many shortcomings and should never be used to establish whether a drug works or not. All doctors know (or should know) this. However, the main point of this post is not to address the claim that hydroxychloroquine is 100% effective against COVID-19, but rather the attitude of scientists towards such claims, especially when they are reported using the media instead of the regular scientific channels. Scientists know that products or therapies that are 100% effective are rare, and this is even more so in the case of major diseases like COVID-19. Some vaccines, hormones like insulin, or a few antibiotics have approached this level of effectiveness, but this is not very common for most other compounds or drugs. About 86% of the drugs tested in clinical trials are found not to be effective and are not approved. Claims of 100% efficacy for a drug or therapy will trigger a strong (and warranted) skeptical response from most scientists.  Quack Quack I have been around a while, and I have read many investigations into multiple bogus claims regarding miracle cures or procedures promoted by quacks. One of the characteristics of these individuals is that they inflate the claims they make regarding the efficacy of their products or therapies beyond the bounds of credibility. If these fraudsters wanted to be believable, they would probably look up the percentage cure rate of the best science-sanctioned therapy and then inflate the claims for their products or therapies by a few percentage points to make them look significantly better but not impossibly so. However, the target audience of these individuals is not scientists but the general public, which has no experience with scientific research or clinical trials and their nuances.
As I have explained before, the best way to promote a bogus product or therapy is to make your audience assimilate your product as part of their identity. If you can achieve this, your audience will be impervious to evidence that the product does not work. This is because any attack on your product will be viewed by the members of your audience as a personal attack on themselves. From this vantage point, it is unfortunate that the president of the United States has promoted the use of hydroxychloroquine. In the current politically charged atmosphere, I am concerned that this identity-forming process seems to be coalescing around the notion that if you don’t accept that hydroxychloroquine works, then you are against the president and thus part of a left-wing conspiracy. It is then all too easy for unscrupulous individuals to exploit this situation by linking themselves to the “pro-president” audience and peddle hydroxychloroquine or other as yet unproven drugs or therapies for COVID-19. If their claims are questioned, all they have to do is argue they are being attacked by the same system that their audience believes is against them and the president. I was skeptical about hydroxychloroquine from the beginning, not because the president promoted it, but because the data for its effectiveness was weak. Thus when I hear these claims for 100% effectiveness of hydroxychloroquine (or any other drug or therapy for that matter), this immediately raises a red flag, and I close my mind to them. This may not seem the scientific thing to do, but remember that keeping your mind too open can be dangerous. As far as I’m concerned, like the late astronomer Carl Sagan said, “Extraordinary claims require extraordinary evidence.”, and the burden of proof is on those individuals who make these claims. It is up to them to produce high-quality evidence to support that what they claim is true, and, seriously, with a 100% success rate this should not prove too difficult, right? At this point you may argue that even if the effectiveness of hydroxychloroquine is less than 100%, but something like 80%, or 50% or 30%, that would still be significant and important. My answer to this is, yes, but this HAS to be established by well-designed clinical trials. At the moment, many clinical trials of hydroxychloroquine are ongoing, and several of these trials are sufficiently well-designed to yield unambiguous results. As I write this, among the best trials completed so far, one has indicated that hydroxychloroquine does not work as a prophylactic against COVID-19, and another has indicated that hydroxychloroquine does not reduce the risk of death among patients hospitalized with COVID-19. The FDA recently revoked its emergency use authorization of hydroxychloroquine, because based on the available evidence it’s unlikely to be effective in treating COVID-19 and any potential benefit from its use outweighs the potential risks. Many of these trials were designed to address the initial claims for hydroxychloroquine being very effective when administered alone or with certain antibiotics. A new claim has been made that hydroxychloroquine is only effective when it is administered with zinc, and new clinical trials are being performed to evaluate this possibility. As I stated above, I am skeptical about hydroxychloroquine, but I don’t want to be right, I want to save lives, and I hope the combination of hydroxychloroquine with zinc works. However, the public has to understand and accept the need to perform clinical trials and stop relying on testimonials and other anecdotal evidence. Image of a quack doctor selling remedies from his caravan; satirizing Gladstone's advocacy of the Home Rule Bill in Parliament is a Chromolithograph by T. Merry, 1889, and comes from the Welcome Collection. The image was modified and used here under an Attribution 4.0 International (CC BY 4.0) license, and no endorsement by the licensor is implied.
0 Comments
 Stay at Home Stay at Home There is a tsunami of misinformation being circulated about COVID-19, and many science communicators are trying to counter this with facts. I have already explained, for example, that COVID-19 is not like the flu, and the perils of ignoring this have already been exposed by the situation of Brazil whose president, Jair Bolsonaro, considers COVID-19 to be “a little flu”, and has done his best to undermine the efforts at mitigation by cities and states in his country. As a result of this, Brazil's COVID-19 cases have jumped to second place in the world after the United States. Another misinformation that is being circulated in social media is the notion that all the mitigation measures against COVID-19, from masks and social distancing to the stay at home orders, did not work to contain the spread of COVID-19. This can be demonstrated not to be true. There is abundant evidence that mitigation against COVID-19 reduced its spread both in the United States (for example: 1, 2, 3, 4, 5, 6, 7, and 8) and in other countries (1, 2, 3). There also is evidence from the past that these measures work. Even if you are not a scientist, it’s not difficult to figure out that a virus will spread more slowly in a population whose members interact less with each other compared to a population whose members interact more. This is really a no-brainer. Mitigation measures have prevented the health care system from being swamped with hospitalizations (what is known as “flattening the curve” of viral spread) as happened in populous localities that did not implement these measures soon enough. You have all read the stories and seen the pictures and videos of what uncontrolled spread of COVID-19 can do. I don’t need to belabor this point. But there are other important things that we have gained with mitigation that are not often mentioned.
There is a vast world-wide network of hundreds of thousands of scientists that has been working around the clock during the pandemic in hospitals, universities, companies, and other organizations investigating the virus, how it spreads, and meticulously analyzing the symptoms of the patients presenting with the disease. These scientists share findings, information, ideas, and experience, and test old and new treatments on cultured cells, animals, and humans. It is thanks to the action of these scientists that we now have a more accurate picture of the symptoms of COVID-19 and effective strategies to minimize the spread of the virus as we rescind stay-at-home orders and begin reopening our society. These scientists are also developing vaccines against COVID-19 and dealing with some unique problems in vaccine development pertinent to coronaviruses, and they are conducting studies to evaluate the benefit of other potential treatments for COVID-19. All in all, there are currently more than a thousand clinical trials all over the world investigating treatments for COVID-19. In these studies, some treatments that were initially touted as game changers such as hydroxychloroquine have so far not lived up to their initial promise. But other studies have shown more promise, such as that of the antiviral compound remdesivir, which is part of a remarkable story involving two decades of research into coronaviruses. One of the greatest achievements of scientists studying COVID-19 is a reevaluation of what the disease really is. The virus that causes COVID-19 is called “SARS-Cov-2”. This stands for “severe acute respiratory syndrome coronavirus 2”. This is because it was thought that the virus would predominantly infect the airways. But early in the pandemic, doctors in China treating COVID-19 patients made the observation that hospitalized patients were experiencing blood clots. Bloodwork analysis indicated that the patients with the most severe illness were strongly positive for some of the most common indicators of risk of increased clotting. Doctors in other countries also found the same thing. A study with almost 3,000 patients found that indeed, those patients administered anticoagulants survived longer: an effect that was even more striking in the sickest patients. The International Society on Thrombosis and Haemostasis issued a document where they provided an interim guidance to treat patients with COVID-19 based on their coagulation parameters. This and other evidence ranging from the molecular to the clinical, has contributed to shape an emerging theory regarding COVID-19 which proposes that, although the disease starts in the lungs, the virus then proceeds to attack the blood vessels. This theory would explain many of the observations made regarding the particular symptoms of COVID-19, and suggests many new lines of treatment. Apart from flattening the curve and other considerations, by delaying the spread of the virus through mitigation we have gained time and knowledge, and during a pandemic these two things are invaluable. Image from pixabay by Queven is used under a pixabay license. A group of skeptics who deny the severity of the coronavirus and the need for or effectiveness of the lockdown, recently piled up on me on Twitter bombarding me with dozens of tweets presenting their arguments with links and videos that “proved” their point. I decided that it was pertinent to write a blog post to deal with these issues.  Coronavirus Conspiracy Coronavirus Conspiracy Recent results of preliminary antibody titers against the coronavirus in New York State have revealed that an estimated of 14.9% of the residents of the state (24.7% in New York City) have antibodies against the virus, which indicates they have been infected. The skeptics pounced on this and similar data from other places to argue that the true death rate from COVID19 is lower than had been calculated based on confirmed cases (which we knew already). So for example, if this number (14.9%) can be extrapolated to the total US population of 330 million people then 14.9% is 46.2 million people, then with 64,000 deaths so far from COVID19, the true death rate due to the virus is 0.13%. They claim this shows COVID19 is no worse than the flu for which the overall death rate is (as can be calculated from data from the CDC) about 0.13-14%. Thus, they argue, the lockdown was not justified, we harmed the economy for nothing, this whole thing has been a hoax perpetrated by the fake news media, and the so-called experts like Dr. Fauci have egg on their faces. Even if you are not a scientist, I hope you smell a rat in this argument. You have probably seen the social media posts of healthcare workers and residents from places like New York, Italy, and Spain stating that they had never seen something like this before. You may even know some of them. You have also seen the images. Morgues overflowing, bodies piling up, patients lying on the floors in corridors, shortages of personal protective equipment, and overworked health care workers coming down with the illness right and left. These people have dealt with the flu before, and this ain’t no flu. Indeed, in New York and in the U.S. as a whole, there was a spike in deaths compared to the past.
So what’s going on? First of all, the influenza cases presented in the CDC website are the influenza illnesses that show symptoms. This is important because as much as 50% of the influenza infections may be asymptomatic which indicates that the true number of infections, and therefore the true influenza death rates, are overestimated (I have made the mistake of quoting these inflated deaths rates for influenza too). You cannot use one figure derived from antibody titers in a calculation and compare it to another figure derived from symptomatic illnesses. Also, let’s not compare apples to oranges. The death rate in a region will depend on various local factors such as how early mitigation was begun, the population density of the region, how many people introduced the virus to the community, the quality and quantity of the health care, the overall health of the people, etc. Therefore it may be misleading to extrapolate the 14.9% total infection rate derived from antibody titers in samples from the State of New York to the whole country. According to the titer results, 2.9 million people are estimated to have been infected in New York State. If you take into account that New York State had 18,274 deaths, this is a death rate of 0.63 % for COVID19 in New York State. If you take the titer results of a 24.7% infection rate for New York City, which has a population of 8.4 million (2,074,800 infected), and has 12,287 confirmed deaths due to COVID19, that gives you a death rate of 0.59% (and using these death figures is an underestimation due to the time lag between infection and death, and the undercounting of COVID19 deaths). These figures are considerably higher than the flu’s overestimated rate of 0.13-0.14%, which is really closer to 0.04-0.05%. Although calculations from titers and numbers in other regions yield different death rates, all estimates are higher than the flu’s. Be it as it may, the antibody titer estimates are preliminary and there are several problems with the test kits used and the methodology employed to obtain the samples. We don’t know yet what the true number of infected people in the United States is, but we know this. So far we have had 64.000 deaths. If these deaths occurred as a result of even 10% or 20% of the people being infected (an unlikely high number for the country as a whole), that means that there are 90-80% of people who have not yet been infected. Thus there is substantial potential for more infection and more deaths, at least until herd immunity sets in. Depending on the local situation, the only thing protecting many people from COVID19 infections right now is mitigation and/or the lockdown. The only consistent thing about the preliminary antibody data so far is that it has not revealed very high titer estimates, which indicates that the mitigation/lockdown measures have been successful and were needed. And this makes sense, mitigation and lockdowns are working here and in other countries today and have been shown to have worked in the past too. There are also additional things to consider. COVID19 spreads faster than the flu and asymptomatic carriers can spread the disease for a longer time than the flu. Additionally, many people infected in the past with one strain of the flu have cross immunity to current strains of influenza and others have immunity due to the influenza vaccine. This limits the number of people that influenza can infect. On the other hand, COVID19 is a novel virus, and there is no immunity against it in our population. The number of people influenza can infect is limited, while the number of people that COVID19 can potentially infect is much higher (at least until herd immunity sets in). In a population without immunity, mitigation, or lockdown, this virus can spread like wildfire leading to steep increases in the number of infected, hospital admissions, and deaths depending on the quality of the health care system and the overall health of the population. Finally, the SARSCoV2 virus, which produces the COVID19 disease, is different from the flu virus, not only at the level of the virus, but also at the level of the disease. So, it’s not true that COVID19 is no worse than the flu, and it’s not true that social distancing and the lockdown were unnecessary. People who promote this misinformation and spread conspiracy theories are harming our society. However, the majority of people that do this are not evil. In fact, what they are doing is predictable, and we have a good idea why they are doing it. People are being laid off and facing the loss of their livelihood, and these people are genuinely concerned about their future due to circumstances they can’t control. They are angry and afraid for their loved ones and for themselves, and they fear the uncertainty of their economic situation more than they fear the virus. It is understandable that these people will fall for the simple “us vs them” arguments peddled by conspiracy mongers who are essentially selling them snake oil. But I have a message for these people. Spreading misinformation and lies, and protesting irresponsibly with no masks or social distancing is unnecessary. There is no need to smear the truth and be unsafe. The lockdown can’t go on forever, and everyone including those who had anything to do with putting it in place want to end it. We just need to do it in a responsible way that does not lead to a full-fledged second wave of the virus that overwhelms our health care system. Getting involved in the process and working with the system is better than attacking it. Call your representatives, learn about the local situation with respect to COVID19 and how it’s being dealt with, offer to get involved in the process, and contribute ideas to reopening while respecting and heeding the advice of health experts. This is the way to go. Conspiracy sign by Nick Youngson from Picpedia.Org used here with modifications under a Creative Commons 3 - CC BY-SA 3.0 license. Coronavirus image by Alissa Eckert, MS; Dan Higgins, MAM, from the CDC's Public Health Image Library is in the public domain.  The Raising of Lazarus The Raising of Lazarus The drug hydroxychloroquine is being tested against COVID19, but there is still no compelling scientific evidence that it works, let alone that it is a “game changer” in our fight against COVID19. However, the president has claimed that there are very strong signs that it works on coronavirus, and the president’s economic adviser, Peter Navarro, has criticized the infectious disease expert, Dr. Anthony Fauci, for questioning alleged evidence hydroxychloroquine works on COVID19. The French researcher, Dr. Didier Raoult, who performed the original trial of hydroxychloroquine that generated all the current interest in the drug, now claims that he has treated 1,000 patients with COVID19 with a 99.3% success rate. In the news, I have read descriptions of patients that have recovered after being administered hydroxychloroquine in what has been called a “Lazarus effect” after the Biblical story where Jesus brought Lazarus back from the dead. So what is a scientist to make of this? I have acknowledged that science cannot operate in a vacuum. I recognize something that Dr. Fauci has also recognized, and that is that people need hope. However, as Dr. Fauci has also stated, scientists have the obligation to subject drugs to well-designed tests that will conclusively answer the question of whether a drug works or not. There seems to be a discrepancy between the quality of the evidence that scientists and non-scientist will accept to declare that a drug works, and there is the need to resolve this discrepancy. People anxiously waiting for evidence regarding whether hydroxychloroquine works, will understandably concentrate on patients that recover. Therefore they are more prone to make positive information the focus of their attention. Any remarkable cases where people recover (Lazarus effects) will invariably be pushed to the forefront of the news, and presented as evidence that the drug works wonders. What people need to understand, is that these “Lazarus” cases always occur, even in the absence of effective interventions. We all react to disease and drugs differently. Someone somewhere will always recover sooner and better than others. How do we know whether one of these Lazarus cases was a real effect of the drug or a happenstance? Isolated cases of patients who get better, no matter how spectacular, are meaningless. Scientists look at people who recover from an illness after being given a drug in the context of the whole population of patients treated with the drug to derive a proportion. The goal is then to compare this proportion to that of a population of patients not given the drug. Scientists also have to consider both positive and negative information. For the purposes of determining whether a drug works, patients that don’t recover are just as important to take into account as those that do. What if a drug benefits some patients to a great extent but kills others? Depending on the condition being treated, it may not be justified to use this drug until you can identify the characteristics of the patients that will be benefited by the drug. To do all the above properly, you need to carry out a clinical trial. No matter how desperate people are, and no matter how angry it makes them to hear otherwise, this is the only way to establish whether a drug works or not.  Hydroxychloroquine Hydroxychloroquine Once we accept the need for a clinical trial to establish whether a drug works, another issue is trial design. A trial carried out by scientists is not valid just because it happened. There are optimally-designed trials and suboptimal or poorly designed trials. There are several things a optimally designed trial must have.
1) The problem with much of the evidence regarding hydroxychloroquine is that it has been tested against COVID-19 in very small trials, and clinical trials of small size are notorious for giving inaccurate results. You need a large enough sample size to make sure your results are valid. 2) Another problem is: what you are comparing the drug against? Normally, you give the drug to a group of patients, and you compare the results to another group that simultaneously received an inert dummy pill (a placebo), or at least to a group of patients that received the best available care. This is what is called a control group. In many hydroxychloroquine trials there were no formal control groups, but rather the results were loosely compared to “historical controls”, in other words, to how well a group of patients given no drug fared in the past. But this procedure can be very inaccurate as there is considerable variation in such controls. 3) Another issue is the so called placebo effect. The psychology of patients knowing that they are being given a new potentially lifesaving drug is different from that of patients that are being treated with regular care. Just because of this, the patients being given the drug may experience an improvement (the so called placebo effect). To avoid this bias, the patients and even the attending physicians and nurses are often blinded as to the nature of the treatment in the best trials. Most hydroxychloroquine studies were not performed blind. 4) Even if you are comparing two groups, drug against placebo or best care, you need to allocate the patients to both groups in a random fashion to make sure that you do not end up with a mix of patients in a group that has some characteristic that is overrepresented compared to the other group, as this could influence the results of the trial. Most hydroxychloroquine studies were not randomized. These are but a few factors to consider when performing a trial to determine whether a drug works. These and other factors, if they are not carefully dealt with, can result in a trial yielding biased results that may over or underestimate the effectiveness of a drug. Due to budget constraints, urgency, or other reasons, scientists sometimes carry out very preliminary trials that are not optimal just to give a drug an initial “look see” or to gain experience with the administration of the drug in a clinical setting. But these trials are just that, preliminary, and there is no scientific justification to base any decision regarding the promotion of a drug based on this type of trials. The FDA recently has urged caution against the use of hydroxychloroquine outside the hospital setting due to reports of serious heart rhythm problems in patients with COVID-19 treated with the drug. A recent study with US Veterans who were treated with hydroxychloroquine found a higher death rate among patients who were administered the drug (to be fair, this study was retrospective and therefore did not randomize the allocation of patients to treatments, so this could have biased the results). Even though I am skeptical about this drug, I would rather save lives than be right. I really hope it works, but the general public needs to understand that neither reported Lazarus effects nor suboptimal clinical trials will give us the truth. The 1310-11painting The Raising of Lazarus by Duccio di Buoninsegna is in the public domain. The image of hydroxychloroquine by Fvasconcellos is in the public domain. For years those opposed to vaccination (antivaxxers) have peen plastering social media with their claims that vaccines are harmful, unnecessary, and ineffective. I had addressed the antivaxxer’s claims before, but I recently had a harsh exchange with some of these people on Twitter. These individuals bombarded me with links to articles and other evidence that “proved” their position was true. After I spent several days going over all this evidence, I found that the vast majority of it was nothing more than a mishmash of mediocre science, innuendo, exaggeration, distortion, and lies. So I organized all the evidence to address their claims. I started writing what I expected to be a two or three part blog post exposing the inaccuracy of the antivaxxer’s claims. However, besides getting me into another fight, I realized my effort wouldn’t really convince anyone that antivaxxers where wrong. I sensed the vaccine issue for most people hinged on more emotional rather than rational variables, and antivaxxers had proven particularly adept at stoking the fears of people and manipulating their emotions.  For years antivaxxers had thrived due to the fact that our society had become complacent. Today’ parents have never had to live with the horrors of smallpox, polio, diphtheria, whooping cough, tetanus, and other diseases. Even though antivaxxers are a minority, they were vocal and organized. They generated enough doubt in our society to give rise to vaccine hesitancy where parents delay or even refuse to administer some vaccines to their children. Predictably, some of the most contagious diseases like measles started coming back. A few antivaxxers thought that the possibility of a world without vaccines was within their reach, and they sought to articulate for others how that world would look. As it turns out, that was unnecessary. If anybody ever wondered how the world would look without vaccines, the COVID19 pandemic has made it abundantly clear how the world looks without ONE vaccine. As I write this, the worldwide confirmed cases of COVID19 exceed two million with more than 169,000 deaths, and more than 700,000 of those cases and 41,000 of those deaths are in the United States alone. Cities, states, and entire countries on lockdown, health care systems overwhelmed, and economies devastated. If anyone harbored any type of misgiving about the need for vaccines, that doubt has been vanquished. And COVID19 is not going to go away anytime soon. There are likely to be waves of the virus as a result of reintroduction when social distancing measures are eased. If sufficiently high numbers of people become infected and recover, a degree of what is called herd immunity may be able to protect those who have not been infected. However, only a vaccine will confer total immunity against the virus. There are currently around 41 research groups and companies in the race for a vaccine, and the hope is that one of these will prove sufficiently safe and effective to neutralize the COVID19 threat for the long-term.
Now that everyone has had a first-hand emotional experience of what a disease can do without a vaccine, I fully expect the antivaxxer influence to wane in our society. I am also planning not to write those blog posts rebutting the antivaxxer’s arguments, as they have become moot and are now a waste of my time. But there is one thing that I do have to point out, and that is the damage that antivaxxers have caused, but not just the one related to vaccine hesitancy or the wasting of resources investigating nonexistent connections between things like vaccination and autism. Vaccines are safe, but they are not risk-free. While being vaccinated is safer than risking having the disease, there are a very small percentage of individuals that will exhibit serious adverse side effects as a result of a vaccine. As vaccines are applied to hundreds of thousands, there will always be a chance that someone with an unknown susceptibility or condition will experience a serious reaction to a vaccine. Here is where antivaxxers could have made a difference for the greater good of society. They could have accepted the effectiveness and safety of vaccines and the need for them, while at the same time advocating for researching vaccine side effects and defining the characteristics of the susceptibility of individuals to developing adverse effects to vaccination. But instead of becoming advocates, they chose to become opponents. Antivaxxers sought out every possible side effect of a vaccine to paint it in the worst possible light. The interest that should exist in the side effects of vaccines has become linked to the antivaxxer position giving it a social stigma. Many people who accept the need for vaccines, but who are genuinely interested in studying and defining the side effects of vaccines, have found out to their chagrin that what they do is often associated with opposition to vaccination. How many people have antivaxxers impacted negatively by creating this stigma may never be known. It is unlikely however, that the antivaxxers will let up anytime soon. As the world anxiously awaits a COVID19 vaccine, antivaxxers may not have the influence that they once had. But if there is anything I have learned from arguing with climate change deniers, creationists, and proponents of 911 conspiracies, chemtrails, the flat Earth and other irrational skeptics is that they will move the goalposts. They will rationalize their failure, rework their arguments around any new evidence or situation, and fan new conspiracies. However, now that the sheer lunacy of the antivaxxer’s dream of a world without vaccines has been exposed, I am hopeful that society will not be as receptive to their arguments. The image by TheDigitalArtist from pixabay is free for public use. Although this is a science blog, I often address instances when belief clashes with science. I subscribe to the notion that religion and science have expertise over different areas and should be kept separate as per the concept of non-overlapping magisteria advocated by the late Harvard paleontologist Stephen Jay Gould. But I recognize there will be cases where that separation becomes fuzzy or unworkable. I have made the point several times in my blog that science is the best method we have to discover the truth about the behavior of matter and energy in the world around us, and this is not an opinion. The success of science in discovering how the natural world works is plain for all but the most irrational skeptics to see. However, at the same time I accept that science cannot operate in a vacuum, and we have to contend with the reality of belief. In these trying times when we are in the middle of the coronavirus pandemic, one of the crucial guidelines that scientists have issued to our population is the need for social distancing and avoiding crowds to reduce the spread of the virus. This guideline is derived from our knowledge of how the virus spreads. Because of this I was shocked when I saw the video below. This woman, who had just attended a church gathering where dozens of people hugged and assembled inside, has the firm conviction that the virus won’t infect her, and that she will not give it to others, because Jesus is protecting her. Most people will criticize the belief of this woman and her congregation and view them intellectually in unflattering terms. However, I understand the need that people have for religion, especially during trying times such as the COVID-19 pandemic. In fact this is nothing new. For millennia, human beings have invoked the deity to help them overcome challenges. I also understand that for many individuals, psychological well-being is often as important as physical well-being. This is not to say that all religious congregations have responded in the way this one did. The majority are offering virtual religious services and other activities that follow social distancing guidelines. But there are a substantial number that are still refusing, and these can (and have) become hot beds of virus spread. However, I don’t think this is solely a religious issue. In the United States, there is a distrust of government among many people. Any ordinance that in any way limits freedom is viewed with suspicion. If you include that there is the belief among some religious groups that a war is being waged on Christianity by atheists aligned with liberal organizations that wish to spread socialism and destroy the American way of life, you begin to get the idea of what may really be transpiring behind this opposition to common sense safety rules that interfere with regular worship. To this, of course, you must add the delegitimization of science that has taken place in our society, and the rise of antiscience movements such as those that advocate opposition to vaccination and climate change denial or the acceptance of conspiracy theories ranging from 911 and chemtrails to the flat Earth.  I believe, however, that there are ways to harmonize belief with science. If you look at the video of the woman again, you can see that she is wearing a seat belt. This makes sense, as science has generated evidence that seat belts along with air bags save lives during collisions. The woman probably doesn’t even think about this when she adjusts her seat belt upon entering the car. She also probably doesn’t even consider driving without a seat belt expecting Jesus to protect her in case of a crash. Additionally, the church she attends probably has lighting rods on top of the roof to protect the building and the people inside from lighting. It is likely that no one in the congregation has even considered removing the lightning rods and relying just on their faith in Jesus to protect the church. So there are clearly science-derived safety measures that these people accept. Why not then accept the safety measures against the coronavirus?
While it’s true that, unlike the acceptance of seat belts or lighting rods, the social distancing guidelines impose a serious restriction in their ability to worship, in essence the occurrence of a viral pandemic is not different from a lighting strike: they are both natural phenomena. Car crashes are a more artificial situation, but they can be rationalized in terms of collisions among moving bodies (a physical phenomenon). If these people have accepted, or at least don’t question, the science and the necessity behind seat belts lighting rods and other such safety measures in their daily lives, how can we convince them that the safety measures against the virus are no different? As it turns out, many religious congregations, including some that share the same brand of Christianity as that of the woman in the video, have already taken care of this issue. They argue that God has responded to our prayers to keep us safe by giving us science, and through science we can understand how the world works and react accordingly. Viewed from this vantage point, applying our God-given science to come up with safety guidelines for the coronavirus is no different from applying it to come up with things like seat belts or lighting rods. No conspiracy. No attack on Christianity, No atheism or socialism. Science does not have an ideology. Science is a tool, and it the right hands it can be used for good. Of course, the above argument that God has given us science is a religious argument and therefore outside the scope of science. But if it means having people accept safety measures that will save lives, I am all for it. Rather than condemn and berate these people for their beliefs, I am of the opinion that the best way to proceed is to search for individuals whom these religious denominations will trust, and have them deliver this argument. Then it can be worked out how to adapt the coronavirus safety guidelines to meet the needs of these religious congregations. Image by geralt from pixabay is for public use.  Starship Troopers Starship Troopers The American writer, Robert Heinlein, wrote a controversial military science fiction novel in 1959 entitled, Starship Troopers, in which a militaristic human society in the future is locked in a war with an alien species that are referred to as “arachnids” or “bugs”. The novel has been turned into an excellent 1997 movie with the same title featuring the actor Casper Van Dien. In the movie, after a particularly disastrous engagement during which the human forces suffers hundreds of thousands of casualties, a new commander is installed (Sky Marshal, Tehat Meru), and in her speech to the United Citizen Federation she summarizes her strategy in one sentence, “To fight the bug, we must understand the bug.” There is a lot of anxiety and fear about the coronavirus now, and the most common questions on everyone’s mind are along the lines of “fighting the bug”. For example: “how can I avoid getting it”, “how can we cure infected people”, or “how can we kill it”. These questions are understandable, but the answer to them can only derive from answers to more fundamental questions along the lines of “understanding the bug”, such as “What is the coronavirus?” or “How does the coronavirus work?” Only if we have the answers to these questions will we be able to “fight the bug”. Fortunately, unlike our fictitious human counterparts in Starship Troopers, we already know a great deal about viruses like the coronavirus and how they work, and this information allows us to “fight the bug”. First of all, what are viruses? Imagine something that is not alive, such as a rock, and something that is alive such as a bacterium. What separates life from non-life? A bacterium reacts to its environment, metabolizes nutrients, and reproduces, while a rock doesn’t. But between these two extremes, there is a shadowy realm populated by entities that retain only one crucial characteristic of living things: they reproduce or rather, they replicate. They either make copies of themselves or act as a template to induce changes in other entities to become like them. But to do this, they must gain access to living things. Viruses are denizens of this realm that exists between life and non-life which they share with other peculiar entities such as plasmids, transposons, and prions. However, unlike the bugs in Starship Troopers, viruses are not an alien entity. Over the course of millions of years in our evolutionary history, viruses infected our ancestors several times and the viral genetic information was incorporated into our own. Today about 8% of our genome bears homology to a class of viruses called retroviruses, and proteins with a viral origin have been coopted by our bodies to perform vital functions such as the development of the placenta. Now let’s move on to coronaviruses. There are several coronavirus strains that infect human beings, causing up to a third of upper respiratory tract infections. When infected people cough, the virus spreads in tiny droplets expelled from the mouth. This is a useful piece of information to “fight the bug” and the basis for doctors telling us to practice social distancing, avoid crowded places, cover our mouths when coughing, and isolate ourselves from others when we are sick so we will not infect them. Knowledge of the time it takes for the symptoms of a viral infection to set in, which is about 5-14 days, is also useful to “fight the bug” and is the basis for a quarantine period of 2 weeks for individuals suspected of having been exposed to the virus. The most serious and sometimes lethal coronavirus infections are those of the lower respiratory tract. These can induce severe inflammation (severe acute respiratory syndrome) of the lung structures involved in oxygenation of the blood impairing their function. This is compounded by the propensity of weakened lungs to have secondary infections, such as those by bacteria. Knowing this is vital to “fight the bug”. Secondary infections can be treated with antibiotics, but people with serious infections of the lung need help with breathing. This is why there is a need for ventilators. Although the current coronavirus is a new strain (SARS-CoV-2), coronaviruses are found both in animals and humans, and they have been intensively studied. The coronavirus is made up of a molecule that carries the genetic information to make more viruses (in this case an RNA molecule) surrounded by a coating of lipids (fats) and protein. Whereas the proteins are unique viral proteins, the lipids aren’t. The virus particles obtain these lipids from the membranes of the cells they infect when they bud off from them. The lipids are essential for maintaining viral structure and function. This is another useful piece of information to “fight the bug”. The lipids can be dissolved by soap, thus inactivating the virus. This is why doctors are telling you to wash your hands. People can become infected with the virus if they touch a contaminated surface and then touch their faces. And while the virus can remain active on surfaces for several days, a variety of disinfectants applied to surfaces can easily destroy the virus.  The genetic information of the coronavirus was sequenced and shared around the world early on in the infection. This is another key piece of information to “fight the bug”, as it is used to make tests. Tests allow us to identify who is sick with the disease, isolate that person, and contact all the people with whom they have interacted and check the places they have been. The genetic information can also be used to make vaccines. There are currently 41 research groups and pharmaceutical companies around the world making experimental vaccines against the virus. While a vaccine will not be a short-term solution, it will prevent a situation where recurring waves of the virus return over the years to infect our societies. An approach that can yield results in the short term involves isolating the antibody rich serum from the bodies of people who have recovered from the virus, and administering that to people still fighting the virus. Finally, knowledge of viral biology is being exploited to come up with therapeutic strategies against the virus, and several possible drugs are being evaluated for activity.
The coronavirus pandemic is a serious threat, but as I have written before, thanks to science, we are not as helpless as we were in the past. If Sky Marshal, Tehat Meru, were in charge of dealing with the coronavirus pandemic in our world today, she would probably say that indeed, “We can fight the bug, because we understand the bug.” The photograph by Hadley Paul Garland of the Starship Troopers novel is used here under an Attribution-ShareAlike 2.0 Generic (CC BY-SA 2.0) license. The transmission electron micrograph of a SARS-CoV-2 virus particle (that produces the disease COVID 19) isolated from a patient, was captured and color-enhanced at the National Institute of Allergy and Infectious Diseases (NIAID) Integrated Research Facility (IRF) in Fort Detrick, Maryland, and is used here with modification under an Attribution 2.0 Generic (CC BY 2.0) license. 3/21/2020 How Bad Is the Coronavirus? Aren’t We Overreacting? Is It a Conspiracy? Please Listen to the Scientists!Read NowThere is considerable anxiety regarding the current coronavirus (COVID-19) pandemic. One of the great unknowns is how bad it will be. The worldwide fatality rate for the virus is 4%. Some people say that the total number of cases is being underestimated which inflates death rates. They claim that the COVID-19 pandemic fatality rate will be no worse than that of the seasonal flu (around 0.09%). Therefore it is unnecessary to cancel travel and sporting events, close businesses, or suspend work. Is the response to COVID-19 overblown? Are scientists irresponsibly hyping the disease for the media and the government with ulterior motives? As would be expected from what I explained before in a previous post, there are already several conspiracy theories circulating regarding the virus. As of now, the vast majority of Americans do not know personally any individuals who have contracted COVID-19 or died from the disease. As far as these people are concerned, life seemed to be going on pretty much the same as it always had until the government stepped in and started curtailing their freedom. All they have to go on is what they see and read in the news and science websites. Therefore, they have to accept that what they are being told is true, and they have to trust those who are telling it to them. The problem is that for years these very same people have been told that that scientists are dishonest and have a hidden agenda, that news organizations are biased and peddle fake news, and that the government is not to be trusted. Many of these people have wholeheartedly embraced conspiracy theories. How can individuals who believe, for example, that global warming is a hoax or that vaccines are harmful and unnecessary trust scientists, the news media, or government to relay to them the facts regarding COVID-19? In this post, I will try to do my best to get some points across. 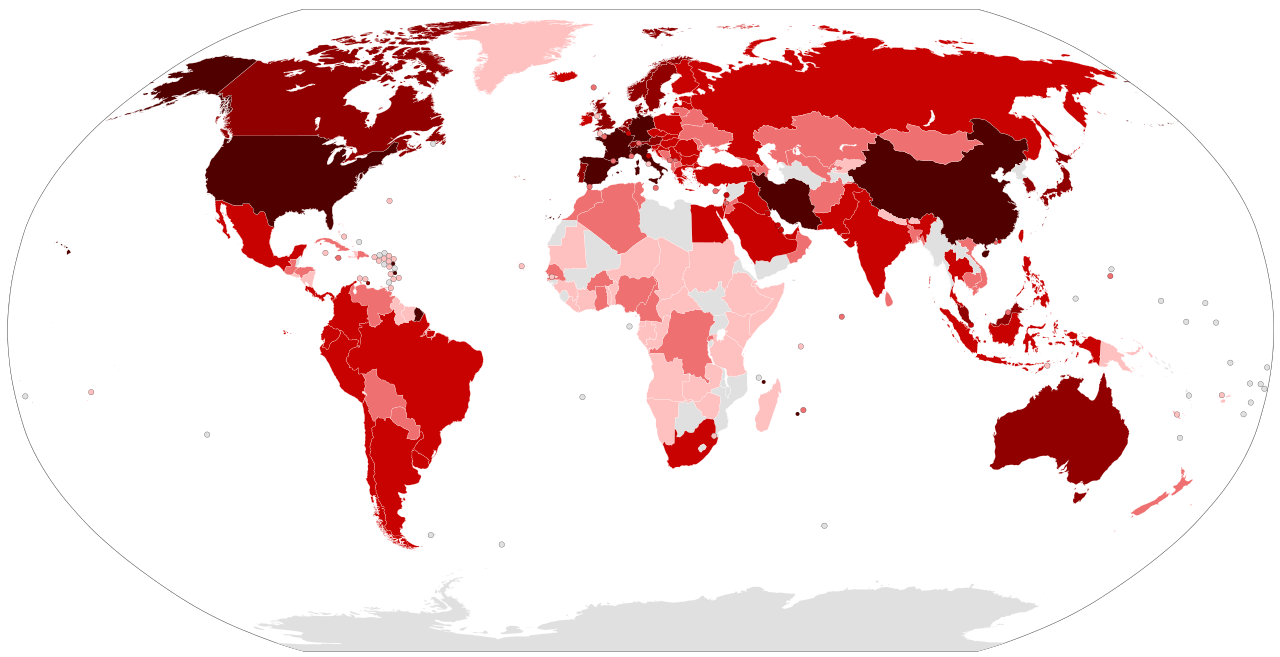 Worldwide Spread of the Coronavirus Worldwide Spread of the Coronavirus As I write this, the worldwide death rate due to COVID-19 is 4% ranging from as high as 8% in Italy to 0.2% in Germany (1.3 % in the United States), and the number of cases is increasing exponentially in some countries. This large variation may be due to many factors such as the makeup of the population and their social characteristics, the quality of healthcare in the country, how early the country responded to the virus, etc. The country that has performed the most tests compared to their total population is South Korea. Although testing has some problems of its own that can result in underestimation of the real number of cases, is likely that South Korea’s numbers regarding the total number of cases of COVID-19 is closer to the real number of total cases. The death rate from the virus in South Korea is 1%, so this lower death rate is probably closer to the “real” death rate of COVID-19. But this figure is still 10 times higher than that for the seasonal flu. It is estimated that the current seasonal flu has infected an average of 46 million American producing 41,000 deaths. If COVID-19, were to infect 46 million Americans, it could produce 460,000 deaths, which is greater than the number of Americans who died during World War II. It must also be stressed that COVID-19 is a new virus. This means that, unlike the seasonal flu, there is no immunity against it in human populations. Also, the ability of the COVID-19 virus to spread in a population seems to be as high as, or even higher than that of the seasonal flu. One final aspect of the disease is hospitalizations and intensive care. In China 15% of the people afflicted with the virus required hospitalization and 5% ended up in intensive care. In Italy the numbers are much grimmer, 50% required hospitalization and 10% ended up in intensive care. By comparison people infected with the flu in the United States have a rate of hospitalization of less than 1.2%. Even if COVID-19 in the United States results in 10% of patients being hospitalized, this level of hospitalizations has the potential to overwhelm the health care system. While older people with preexisting conditions seem to be at higher risk of hospitalizations, so far in the United States 38% of those sick enough to be hospitalized are younger than 55, so that is also a cause of concern. Do you see now why scientists are spooked and are advising the media and the government to report and proceed accordingly? And this is not just scientists in the United States. Scientists from every country in the world are sounding the alarm. These are individuals who have different religious and philosophical beliefs, different political opinions, and come from various ethnic and social backgrounds, but they are all saying the same thing. How can this be a conspiracy? It is true that there are unknowns. It is true that the real effect of the virus may turn out to be milder than expected, but do we want to risk it? Some people complain that in the last pandemic that affected the United States, the Swine flu of 2009, apart from some school closings, no further drastic measures were taken. It must be understood that drastic measures to curtail the spread of a virus will harm the economy and may even cause a recession. Recessions lead to layoffs, they stress individuals and families, and they affect the physical and mental health of the population. Recessions kill and harm individuals and have long lasting consequences. Therefore, drastic measures to curtail the spread of a virus may harm the economy and should not be taken lightly. Early on in the Swine Flu pandemic scientists obtained data that indicated that the virus would not be as bad as it seemed to be initially and recommended against drastic measures to curtail the spread of the virus. The recommendation turned out to be accurate. The Swine Flu resulted in the hospitalization of 0.45% of those affected producing a 0.02% mortality. This mortality still represented 12,500 deaths, but was substantially below those of the seasonal flu. Scientists tell us that we should be concerned about COVID-19 and that we should modify our behavior to protect ourselves and others. They do so based on the best available data, and they inform the news media and advise the government accordingly. What these scientists do is not different from what other scientists are doing raising the alarm about global warming and telling us that vaccines do not cause autism and explaining how important they are in protecting us from disease. Please listen to the scientists! The image of the worldwide spread of COVID-19 from the Wikipedia Commons is used here under an Attribution-ShareAlike 4.0 International (CC BY-SA 4.0) license. We are now in the midst of pandemic of a coronavirus disease called COVID-19 caused by a virus called “severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2), and there is some anxiety regarding certain unknown aspects of this virus. For example, the death rates appear significantly higher than those of the regular flu (note however that COVID-19 is not a flu or even related to the flu), but there is uncertainty as to whether this is due to an underreporting of milder non-lethal cases. However, the majority of deaths seem to occur among older weak people with previous health problems, and infected people that do not yet have symptoms upon viral infection do not seem to be a major driver behind the spread of the virus. Will COVID-19 turn out to be a disease no more serious than the flu, or will it be much worse? In a previous post I quoted the late horror writer, H. P. Lovecraft, who wrote that “The oldest and strongest emotion of mankind is fear, and the oldest and strongest kind of fear is fear of the unknown.” But even as we remain somewhat fearful about what we don’t know regarding COVID-19, we must remember not only what we do know about diseases today and the fact that we have the tools fight them, but also how little we knew about them in the past and how helpless we were. Let’s start with the Black Death. The Bubonic Plague or Black Death ravaged many areas of the world in antiquity. The disease is caused by a bacillus, Yersinia pestis, which infects rats (although other animal hosts are also common) and is then transmitted to humans by fleas that bite infected rats. The most famous outbreak of the plague was that which occurred in Europe from 1347 to 1351 and which wiped out an estimated two thirds of the continent’s population (about 50 million people). Poor public hygiene and crowded living conditions in Europe created an excellent environment for the spread of disease. The role of germs or insects in the causation of disease was unknown, and physicians were helpless against the onslaught of the disease which was blamed on several things ranging from foul air and unfavorable planetary alignments to divine punishment for sins.  Painting of the city of Marseille during the Great Plague Today it is difficult to comprehend the sheer level of terror triggered by the plague in Europe and the breakdown of society and institutions that it caused. Corpses accumulated in the streets. Family members abandoned their dead and dying. Government officials, doctors, and priests deserted their posts. In some cities up to 80% of the population was wiped out. Some rulers instituted draconian measures like boarding up houses with all the occupants inside if one person in the house was infected, thus condemning all those inside to die. Ignorance, superstition, and fear combined to trigger barbaric behavior in mobs of people that targeted and killed individuals or certain groups of people like gypsies or Jews who were rumored to be behind the causation of the plague. Several plague pandemics ravaged Europe over hundreds of years causing the death of millions. It was only in 1894 that the Swiss-French physician, Alexandre Yersin, discovered the plague bacillus and the role of rodents in its spread, and in 1898 the French physician Paul-Louis Simond discovered the role of fleas in the transmission process. This allowed the implementation of effective public hygiene measures that finally controlled the disease. Now let’s move on to the so called Spanish Flu. From 1918 to 1919 an influenza pandemic called the Spanish Flu killed 50 million people in the world and 500,000 in the United States. Due to World War I, any news about the flu that could be used as propaganda by the enemy was censored in many countries including the US, but the general public could tell that something out of the ordinary was going on. Unlike previous flu infections, this strain of influenza mostly affected and killed people in the prime of their life (20 - 40 years old), and it quickly overwhelmed the health care system in many localities which had to resort to interring the dead in mass graves. There was no way to treat influenza or the deadly secondary infections it generated, so fighting the disease consisted on mostly preventive measures such as good hygiene, quarantine, closing venues where large numbers of people congregated, and supportive care for those infected. The fear of the times of the plague returned. Scores of people locked themselves in their houses, refused to help their neighbors, and refused to go to work emptying the streets of some cities and towns. 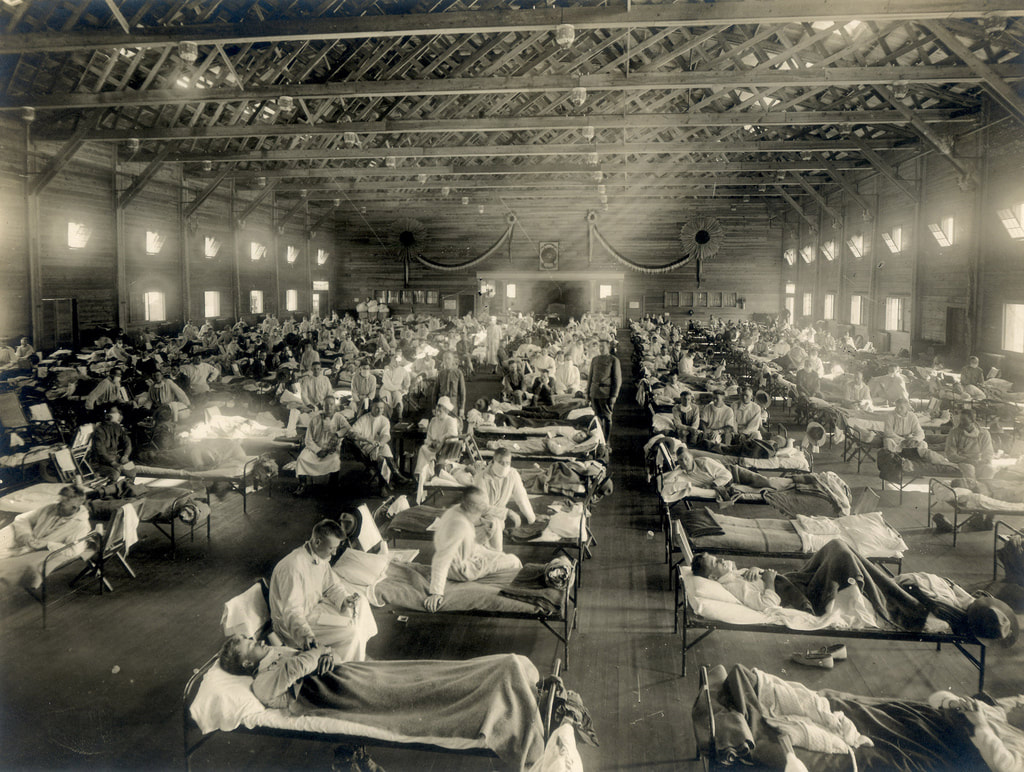 Emergency hospital during influenza epidemic The causative agent of the flu was originally believed to be a very small bacterium, but the development of the field of virology eventually led to the understanding that the flu is caused by viruses. With the invention of the electron microscope in the 1930s, viruses like the ones that cause the flu could be visualized. In 1999 the Spanish Flu virus was recovered from people who died during the pandemic. The virus was reconstructed in 2005 and studied to figure out what made it so virulent. So how do the last two pandemics compare to the COVID-19 pandemic today?  SARS-CoV-2 virus particle which produces the disease COVID 19 SARS-CoV-2 virus particle which produces the disease COVID 19 Unlike what happened with the Black Death or the Spanish Flu, we know exactly what COVID-19 is. We know what the virus looks like, and what it does and how it does it. We have a good idea of where it originated and how. We have sequenced its genome in record time, and used that information to make test kits that permit the identification of those people that are infected, so they can be quarantined and questioned about their contacts and the places they have been. We have antibiotics to treat secondary infections triggered by the virus. We are testing antivirals that may be of use against the virus, and we have also begun to develop vaccines. There is a vast worldwide network of organizations such as the Global Virus Network and the World Health Organization that are tracking the spread of COVID-19 and coordinating the sharing of information among experts in different disciplines at every level and informing the public. There are government agencies such as the Centers for Disease Control and Prevention (CDC) in the U.S. that are monitoring the individual cases in a given country, coordinating the public health response, and advising the government and the general population.
Humanity’s knowledge of disease and its response to it has come a long way since the times of the Black Death and the Spanish Flu. We will continue fearing the unknown, but thanks to science this “unknown” has been made much smaller. Today we fear less. The painting of Marseille during the Great Plague by Michel Serre is in the public domain. The photograph of an emergency hospital during influenza epidemic in Camp Funston, Kansas, circa 1918 is from the National Museum of Health and Medicine, and is used here under an Attribution 2.0 Generic (CC BY 2.0) license. The transmission electron micrograph of a SARS-CoV-2 virus particle (that produces the disease COVID-19), isolated from a patient, was captured and color-enhanced at the National Institute of Allergy and Infectious Diseases (NIAID) Integrated Research Facility (IRF) in Fort Detrick, Maryland, and is used here under an Attribution 2.0 Generic (CC BY 2.0) license. |
Categories
All
Archives
April 2024
|
 RSS Feed
RSS Feed